Thank you for supporting our
2023 LIFE WITHOUT LIMITS Gala!
View our Gala E-Journal here!
Life Without Limits for People with Disabilities™
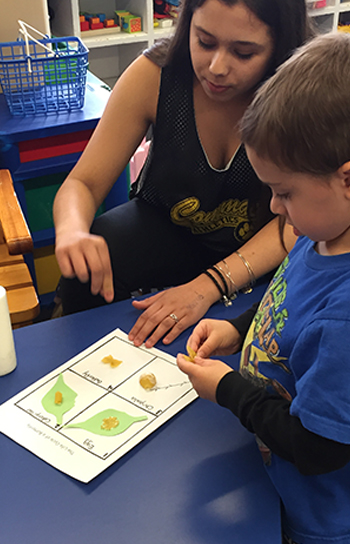
What began in 1950 with a small group of parents seeking support for their children with cerebral palsy has evolved into one of the most far-reaching and successful providers of services to people with a wide range of disabilities on Long Island.
Since its inception, UCP of Long Island has been committed to advancing the independence, productivity and full citizenship of people with disabilities by creating Life Without Limits.
For questions regarding nonprofit organizations contact:
charities.bureau@ag.ny.gov or (212) 416-8401.